Fact Sheet | 15 October | Download PDF
Research carried out in Kenya by Health Action International looked at the impact of coronavirus—and associated measures to prevent its spread—on rural communities in the country.
BACKGROUND OF THE SURVEY
At the time of writing, there have been over 35 million confirmed cases of COVID-19, resulting in over one million deaths worldwide. The pandemic is unprecedented in modern history and coronavirus has spread to every corner of the globe. Research carried out in Kenya by Health Action International looked at the impact of coronavirus—and associated measures to prevent its spread—on rural communities in the country.
In August 2020, a household survey was conducted in two communities from Mwatate Sub-County (n=50) in Taita Taveta County and five communities from Kilifi North Sub-County (n=50) in Kilifi County. Households were selected using a sampling interval of three—i.e., each third, sixth, ninth etc. dwelling in a street were visited. If no one could participate, the neighbouring house was visited.
DEMOGRAPHICS
Survey respondents were 53% male and 47% female. Ages ranged from 19 to 70 years, with an average of 46 years. Most respondents were farmers (35%), shopkeepers or service workers (23%), unemployed (15%), teachers (8%) or civil servants (7%).
EFFECTS OF COVID-19 AND RELATED MEASURES
Only two respondents knew a person who has or has had the coronavirus (2%). However, while the surveyed communities seemed to be little affected by the virus itself, they were greatly affected by its consequences. A striking 96% of respondents identified loss of income as a major issue in their community after the public measures against COVID-19 came into effect.
Over half (56%) of respondents reported that their own household had lost income. Respondents mostly attributed their households’ loss of income to: loss or lay-off of jobs (29%), loss of business, sales or work activities (25%), delayed salaries (11%), lack of money or money circulation (11%), closure of business or market (9%) and reduction in salaries (5%). In addition, 51% of respondents found lack of food to be a problem in their community since COVID-19 measures were put in place and another 21% reported lack of access to water for handwashing.
Thirteen percent of respondents knew someone who had not been able to access a health service due to COVID-19 measures. The most important reason was that the person did not visit a health facility because of fear of contracting the coronavirus (n=10).
Reasons mentioned in single cases were that the health facility was not providing this service due to the coronavirus, there was no healthcare worker to serve them and lack of money to purchase the service. Five percent of respondents knew someone who could not get medicines due to the COVID-19 measures. Reasons mentioned were again fear of contracting the coronavirus, and in single cases: lack of transport, unavailability of the medicine, and lack of money to purchase it.
Incidents of violence or aggression in the community since the COVID-19 measures were reported by 15% of respondents. Examples mentioned were police harassment or brutality, insecurity, theft, and family arguments.
INFORMATION AND KNOWLEDGE
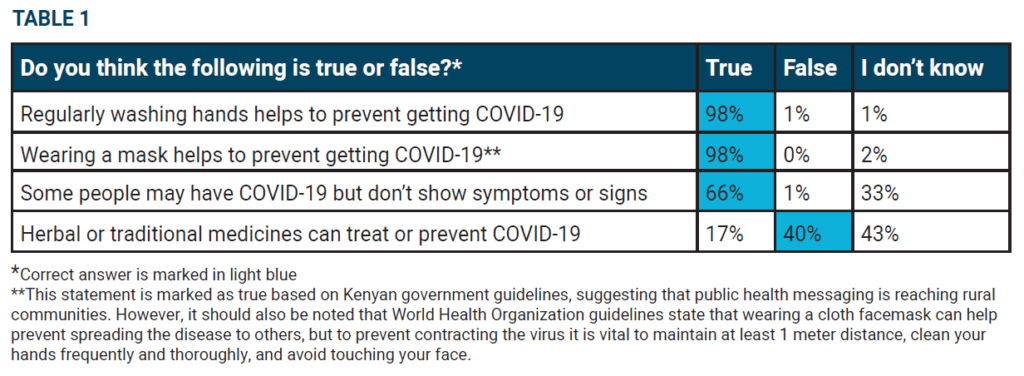
Respondents generally had a high trust in information from health authorities about COVID-19, as only 1% believed this information was unreliable or very unreliable. Also, many respondents found information provision to be sufficient, with 94% of respondents stating they had enough information about COVID-19. Knowledge about handwashing and Kenyan
government guidelines on wearing of facemasks was very good.
Knowledge about the possibility of having COVID-19 asymptomatically and the effectiveness of herbal or traditional medicine to treat or prevent COVID-19 presented a more mixed picture (see Table 1).
STIGMA AND FEAR
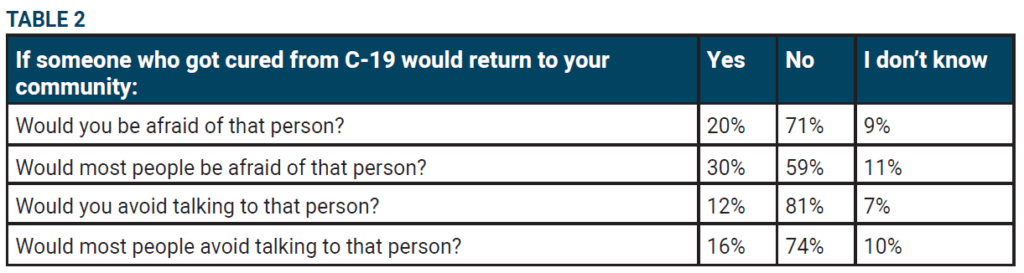
Respondents were asked how they would feel if someone who had recovered from COVID-19 would return to the community. Some respondents reported they would be afraid of the person (20%) and would avoid talking to the person (12%), but fortunately, the majority of respondents said they would not be afraid or avoid conversation (71% and 81%, respectively) (see Table 2).